![Diseases, Symptoms, tcm, [tcmwindow.com]](/uploadFile/adImg/2015/11/11/f5cbfcc0-4df5-4646-9b9a-f316651a0199.jpg)






Acupuncture restores normal swallowing in post-stroke patients and investigators document an optimal approach to patient care. Researchers find low frequency electroacupuncture more effective than high frequency electroacupuncture for the relief of post-stroke dysphagia (difficulty or discomfort in swallowing).
Guangzhou University of Traditional Chinese Medicine researchers combined acupuncture with general health care and rehabilitation exercises into an integrated treatment protocol. They conclude that acupuncture is effective for the treatment of post-stroke dysphagia and that patients receiving low frequency electroacupuncture had superior patient outcomes compared with patients receiving high frequency electroacupuncture. The total effective rate in the low frequency group was 93.3%. The total effective rate in the high frequency group was 66.7%. The low frequency group outperformed the high frequency group by 26.6% (P<0.05).
Difficulty with swallowing is a common complication caused by strokes. If not identified and managed, dysphagia leads to poor nutrition, pneumonia, or increased disability. For most stroke patients, swallowing function recovers within 48 hours. However, if it fails to recover within 2 weeks, the dysphagia often continues beyond 70 days.
The Traditional Chinese Medicine (TCM) classic, the Su Wen (Plain Questions), prescribes targeting the Ren and Du meridians for the treatment of dysphagia, "the Du meridian starts from the perineum . . . it ascends inwardly through the lower abdomen, umbilicus, and heart, reaches the throat and curves around the lips. . . . the Ren meridian, which runs up the front of the body, starts below Zhongji (CV3), ascends superficially through the abdomen and chest to the throat, and intersects the Du meridian around the mouth." Administering acupuncture along these meridians regulates qi and blood circulation, corrects the imbalance of yin and yang, and works to eliminate dysphagia.
According to the investigators, common acupoints used for the treatment of post-stroke dysphagia include Lianquan (CV23) and Fengfu (GV16). The Lianquan (CV23) acupoint is located on the Ren meridian; this acupoint is traditionally indicated for difficulty with swallowing and aphasia. In a related finding, researchers note that needling Lianquan (CV23) "triggers swallowing-related activities through regulating the discharge of swallowing-related neurons in the nucleus of the solitary tract (NST)."
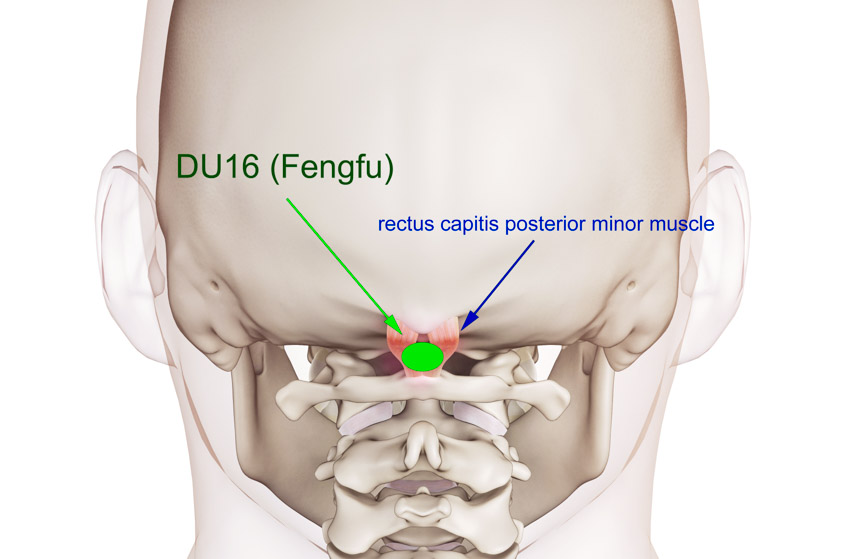
Fengfu (GV16) is located on the Du meridian; this acupoint is also useful in treating oral and pharyngeal disorders. Modern research has proven that needling this acupoint "activates swallowing-related neurons in NST." Researchers from Guangzhou University of Traditional Chinese Medicine (Wang et al.) tested both Lianquan (CV23) and Fengfu (GV16) in a controlled experiment and confirm that it is effective for recovery from difficulty swallowing. The investigation focused on brain repair following a stroke due to cerebral ischemia. In the experiment, needling these points has shown bilateral activation of the brain’s swallowing motor cortex and heightened plasticity of the post-ischemic region of the brain.
Design
The researchers (Zhang et al.) used the following study design. A total of 60 patients were treated and evaluated in this study. The patients were diagnosed with post-stroke dysphagia between June 2015 and January 2017. They were randomly divided into a low frequency electroacupuncture (EA) group and a high frequency EA group, with 30 patients in each group. For the low frequency EA group patients, EA at 2 Hz, general health care, and lingual exercises for dysphagia rehabilitation were given. The high frequency EA group received EA at 100 Hz in addition to the identical health care and rehabilitation treatment administered to the low frequency group.
Prior to treatment, the statistical breakdown for each randomized group was as follows. The low frequency group consisted of 16 males and 14 females. The average age in the low frequency group was 60 ±11 years. The average course of disease in the low frequency group was 29 ±3 days. The high frequency group consisted of 15 males and 15 females. The average age in the high frequency group was 59 ±9 years. The average course of disease in the high frequency group was 22 ±4 days. There were no significant statistical differences in gender, age, and course of disease relevant to patient outcome measures for patients initially admitted to the study.
Health Care
For both groups, patients received identical general health care and rehabilitation exercises. General health care involves allopathic medicinal treatments for hypertension, diabetes, and heart disease. Lingual exercises were also performed to restore glossopharyngeal muscle function and tongue sensations. The rehabilitation exercise was conducted daily for 30 minutes for a total of 14 consecutive days.
Acupuncture
Both groups received electroacupuncture therapy but with different frequencies. For the low frequency group, a 2 Hz frequency electroacupuncture was administered. For the high frequency group, a 100 Hz frequency electroacupuncture was administered. The acupoints used included the following:
CV23 (Lianquan)
GV16 (Fengfu)
For Lianquan, treatment commenced with patients in a seated position. After disinfection of the acupoint sites, a 0.35 mm x 40 mm disposable filiform needle was inserted into the acupoint with a high entry speed, at an entry direction towards the root of the tongue, to a depth of 16 – 30 mm. Next, the Ping Bu Ping Xie (attenuating and tonifying) manipulation technique was applied until the needle stimulated a strong deqi response towards the root of the tongue.
For Fengfu, treatment commenced with patients in a seated position. The patients were asked to bend the head slightly forward to relax the neck muscles. After disinfection, a 0.35 mm x 40 mm disposable filiform needle was inserted downwardly into the acupoint with a high needle entry speed, reaching a depth of 16 – 26 mm. An upward needle entry direction is strictly prohibited. That is a contraindicated needling technique because it might insert the needle deeply into occipital foramen and reach the medulla oblongata. It is for this reason that only licensed acupuncturists are advised to administered this procedure.
After needle insertion, an electrotherapy device was connected to the needles and set to a continuous frequency (2 Hz for the low frequency group and 100 Hz for the high frequency group), for 30 minutes. One 30 minute acupuncture session was conducted daily for consecutive 14 days.
Evaluation
Evaluations were performed before and after the treatment with the help of multiple instrumental assessment tools:
Video Fluoroscopic Swallowing Study (VFSS)-this is the current gold standard for the diagnosis and management of dysphagia. The following three aspects were scored: food passage time in the oral phase, food delay time in the pharyngeal phase, and food passage time in the pharyngeal phase.
Water-Swallowing Test (WST)-this is commonly utilized in clinical practice to evaluate swallowing function.
Standardized Swallowing Assessment (SSA)-this is an additional tool used to determine the nature and extent of a swallowing disorder.
For VFSS, food passage time in the oral phase, food delay time in the pharyngeal phase, and food passage time in the pharyngeal phase was lower than before treatment in both groups (P<0.05). The results in the low frequency EA group were better (P<0.05) than in the high frequency group. The WST score improved in the two groups (P<0.05). Again, the low frequency group outcomes were significantly better (P<0.05) than in the high frequency group. The SSA score decreased in the two groups (P<0.05) and the improvement in the low frequency group was significantly superior to that in the high frequency group (P<0.05).
Results
The results indicate that acupuncture combined with general health care and rehabilitation exercise into an integrated treatment protocol is effective for the treatment of post-stroke dysphagia. In addition, 2 Hz electroacupuncture produces higher effective rates than 100 Hz electroacupuncture when implemented in the integrated treatment protocol. Zhang et al. conclude that acupuncture is safe and effective for the relief of post-stroke dysphagia.
References
[1] Zhang LZ, Xu NG, Li RL, Wang L. Clinical Study of Electroacupuncture with Different Frequencies at Lianquan (CV 23) and Fengfu (GV 16) for Stroke Dysphagia [J]. Chinese Acupuncture & Moxibustion, 2018,38(02):115-118.
[2] Liu XH, Liu AZ, Zhang XL, Du L, Hu H, Li L, Jiang GD, Chen N, et al. Clinical Observation on Acupuncture Treatment of Pseudobulbar Paralysis [J]. Chinese Acupuncture & Moxibustion, 2000(06):5-8+4.
[3] strokeassociation.org
[4] Hamdy S, Aziz Q, Rothwell JC, et al. Explaining oropharyngeal dysphagia after unilateral hemispheric stroke[J]. Lancet, 1997, 350(9079): 686-692.
[5] Zhao JY. Regulation of Acupuncture Ren and Du Meridian on Regulating Swallowing Intermediate Neurons [D]. Guangzhou TCM University, 2015.
[6] Sun WP, Huang YN, Wang Z et al. Value of Standardized Swallowing Assessment in Screening for Aspiration after Stroke [D]. Guangzhou TCM University, 2016.